Urinary tract stone disease is the most common problem of excretion system after urinary tract inflammations and prostate diseases. An increase has been reported in the incidence of kidney stones during the past 20-30 years. While the obvious reason behind this elevation is not known, it is attributed to changes in dietary habits and lesser fluid intake.

How does a kidney stone form?
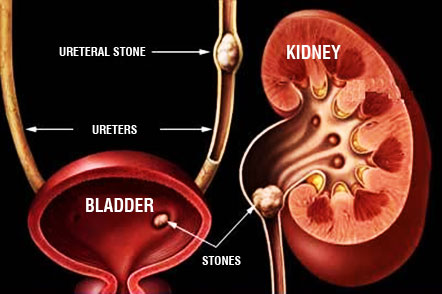
Kidneys work as the filter system of our body. Blood is always filtrated in the kidneys whereas beneficial substances are absorbed and unwanted substances are excreted with urine. Presence of a urine with high-concentration, elevates the risk for formation of kidney stone. Salts and minerals excreted with the concentrated urine, generate accumulations which later turn to stones in the tubular units localized in the inner surface of the kidneys. In time, those crystals come together and form a stone.

Kidney stone disease (nephrolithiasis) occurs as a result of high level of calcium (hypercalciuria), oxalate (hyperoxaluria) or uric acid (hyperuricosuria) and due to low citrate levels which reduce the adhesion of crystals, and inadequate fluid intake. This process may be considered similar to the transformation of a single sand grain into a pearl in time. The size of the stones may vary from a little rice grain to a mandarin.
What are the complaints associated with kidney stones?
Majority of the kidney stones do not display any signs and are detected during radiological examinations performed for other purposes. If the stone has a large size and obstructs renal pelvis, then it may cause pain. As the stone moves into the duct between bladder and kidney, it may completely obstruct urine flow and lead to a severe pain termed as colic. The pain originates from waist level and spreads through the thighs along with possible additional symptoms such as nausea, vomiting, or abdominal distension. Hematuria may be present due to irritation of the urinary tract because of the stone.
How is kidney stone diagnosed?
Some kidney stones are diagnosed accidentally. By inclusion of USG in check-up programs, currently the number of kidney stones diagnosed before causing any symptoms, is on the rise. On the other hand, major symptoms that bring patients to physicians are known to be low back pain, recurrent urinary tract inflammation, and hematuria. Patients presenting with those symptoms can be diagnosed by application of the following examinations.
• Direct Urinary System Radiography (DUSR): By using x-ray, most of the opaque kidney stones can be detected. Non-opaque or small stones can not be determined with this technique.
• USG: High-frequency sound waves are utilized for visualization of the internal organs and the data are reflected on a display by the help of a computer. While it seems to be a safe method due to absence of x-rays, it proves to be inefficient particularly in detection of small stones in the ureters.
• Intravenous Pyelography (IVP): Both anatomy and function of kidneys can be examined by intravenous delivery of a contrast agent. Detailed information on localization of the stones in the kidney and the damage they inflicted can be obtained. This technique should not be performed on people who are pregnant or suffer from renal failure and allergy against the contrast agent.
• Spiral Computed Tomography (CT): Currently, thin section urinary CT has become the gold standard for assessment of kidney stones. The assessment can be performed within minutes and even milimetric stones can be detected.
Should other analyses be applied on patients diagnosed with kidney stone?
Studies show that recurrent stone formation is observed in 50% of cases in a 5-year period where no preventive measures are taken against stone formation. In order to prevent this, among patients who display recurrent stone formation or demonstrate a predisposition, certain preventive measures should be taken. In order to perform this analysis which is called metabolic assessment, 24-hour urine samples are collected and calcium, uric acid, citrate, and oxalate levels are measured. By collecting a blood sample at the same time; blood calcium, inorganic phosphate and parathormon levels are determined, as well.
What are the factors that elevate the risk of kidney stone formation?
If we are to list those respectively:
• Inadequate fluid intake: Failure to intake adequate fluid, particularly water, the concentration of minerals leading to stone formation rise. Therefore, people living in hot climates or working in hot environments are under greater risk for stone formation.
• Family history and personal history: The risk of stone formation is higher for people whose families have a stone history. Also, a person who had experienced stone formation once in kidney, has a 50-60% risk to redevelop it in the following 5-year period.
• Age, gender and race: Kidney stone is commonly encountered between the ages of 30-50 range. It is more frequently seen in males and white people.
• Certain diseases: Rare diseases such as renal tubular acidosis, goutte and cystinuria increase the risk for stone formation.
• Diet: Diets containing high animal proteins and low fiber content elevate the risk for stone formation. Moreover, excessive salt consumption has been associated with stone formation, as well.
• Inertia or low activity: Bedridden patients and patients who display low activity may suffer osteoporosis which leads to elevation of calcium levels in the urine and therefore puts the patient under high risk for stone formation.
Should kidney stones be treated?
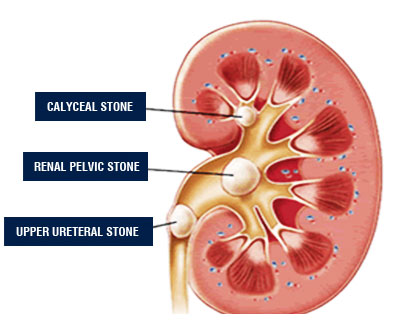
Stones localized in the renal pelvis should be treated. Otherwise, they can cause dysfunction or inflammation in the kidney.
Generally, stones in the calyces of kidney display a latent course and does not lead to a problem. But caliceal stones can grow in situ or move into the ureter and cause complaints such as pain or inflammation. Therefore, caliceal stones should be treated.
How does the kidney stones treated?
Medical Treatment
Stones with less than 5mm diameter can be treated with plenty of water consumption and drug therapy. The possibility of passing out larger stones is very low.
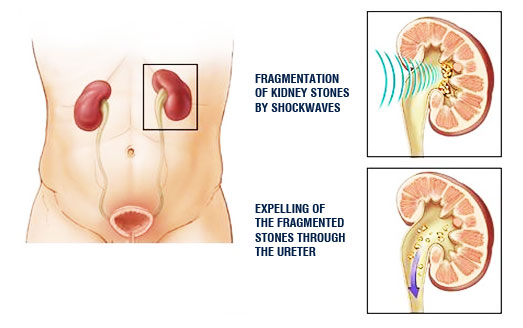
ESWL (Extracorporeal Shockwave Lithotripsy)

This is the most common method applied in treatment of kidney stones. Shockwaves generated outside the body are directed onto the stones to fragmentate them. Then, those pieces are passed out in the urine. In order to reduce the pain during procedure, sedative drug or a mild anesthesia may be required. Expelling of stones following ESWL may take days or even weeks. Patients may feel pain and develop urinary tract inflammation. Although rare, sands may accumulate in the ureter and the expelling may be delayed which requires an additional treatment.
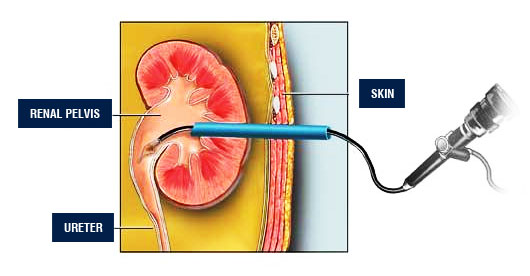
Percutaneous Nephrolithotripsy (PNL)
This is one of the current methods which is applied when ESWL fails to fragmentate the stone or have a size above 2cm. By reaching the kidney through a 1cm incision from the lumbar region under general anesthesia, stones are removed via the same route as a whole or in fragments. During percutaneous nephrolithotripsy, an endoscopic i.e. closed operation, images are transferred to a display screen by an endocamera. Stones are fragmentated mostly with pneumatic, ultrasonic or laser devices. At the end of the operation, a nephrostomy tube is temporarily placed into the kidney in order to void the urine for the following 2-5 days.
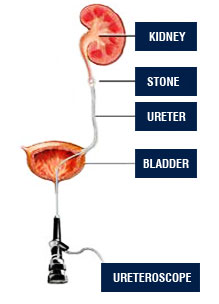
Ureteroscopy
In case expelling stones from the ureter or breaking them up with ESWL fails, those patients can be treated by insertion of an instrument called ureteroscope. Ureteroscopes are of 2.5-3 mm diameter and have a tube allowing to perform various procedures and a lense system. Rigid (inflexible) ureteroscopes are inserted through urethra and bladder into the ureter and treatment is applied by fragmentating stones with Holmium laser or pneumatic lithotriptor. Stones in the lower and midureter can be treated with ureteroscopes. Flexible ureteroscopes are employed in treatment of stones localized in the upper ureter or renal pelvis and calyces due to their ability to be rotated in different directions at different angles. Patients can be discharged overnight or 1 day after the ureteroscopic stone treatment.
Can the formation of kidney stone be prevented?
By making few changes in the nutrition and life style, the risk of stone formation can be reduced. Earlier diets including strict limitations have been shown to be ineffective due to difficulty to follow. Patients should be encouraged to take high volumes of fluid. This is a valid recommendation against urinary tract stones regardless of the composition of the fluid. The daily urinary volume of an adult person should be above 2 liters. Fluid intake should be distributed throughout the day evenly and particular attention should be paid in case of fluid loss.
A mixed and balanced dietary program is needed in all patients. Fibrous foods and vegetable-fruit consumption should be encouraged. However, vegetables-fruits that are rich of oxalate (spinach, cacao, tea leaves, walnut, and bran) should be avoided. This is important especially for patients who exhibit high level of oxalate in their urine.
C vitamin may be taken 4g/day without elevating the risk for stone formation. Animal proteins should not be consumed excessively. Animal protein consumption should be limited to 150g/day. Calcium intake should be limited unless there is a reasonable cause. Required daily calcium consumption is 800mg and generally 1000mg is recommended. Calcium supplement is recommended only if there is enteric hypocalcuria.
In hyperuricosuric calcium oxalate stone disease, and among patients with uric acid stone, consumption of foods rich of urate (liver, kidney, skin of poultry animals, skin of herring fish, sardine, and anchovy) should be limited. Urate amount per diet should not exceed 500mg/day.
Currently used Diet for Prevention of Stone Formation is simplified and summarized below.
- Adequate fluid intake should be maintained.
- Fluid intake should be enough (e.g: 3 liters/day) to produce a daily urine output of 2 liters. Considering that one glass of water is comprised of 200cc., we should drink about 15 glasses of water.
- Tea and milk should be excluded in calculation of total fluid intake whereas at least half (8 glasses) of the whole fluid intake has to be water and should be distributed evenly throughout the day. Fruit juices are recommended alongside water.
- Another important point on maintaining a fluid balance is to keep the fluid level balanced in the sleep hours during which urine gets more concentrated due to absence of fluid intake. Therefore, the fluid intake volume should be elevated by considering the sleep hours.
- Less salty foods should be preferred.
- Excessive consumption of foods that are rich of animal proteins (meat and meat products, milk and dairy products, egg etc..) should not be consumed. If possible, limit consumption of those foods to only 1 meal.
- Calcium-rich foods should not be consumed excessively. Moreover, one should be aware that calcium-rich foods are generally rich of animal proteins, as well.